Why ApoB is more accurate than LDL cholesterol
Last updated March 2026
When it comes to predicting your attack risk, the two most common blood markers are LDL cholesterol and apolipoprotein B (ApoB). While LDL has long been the standard, a growing body of evidence (and recent international guidelines) show that ApoB predicts cardiovascular disease better than LDL. In a 2025 scientific review, 9 of 9 studies showed ApoB is more accurate than LDL cholesterol.
According to Allan Sniderman, Professor of Cardiology at McGill University, if you measure ApoB and Lp(a), you get better information about your heart disease risk than by measuring LDL cholesterol, triglycerides, cholesterol particle sizes:
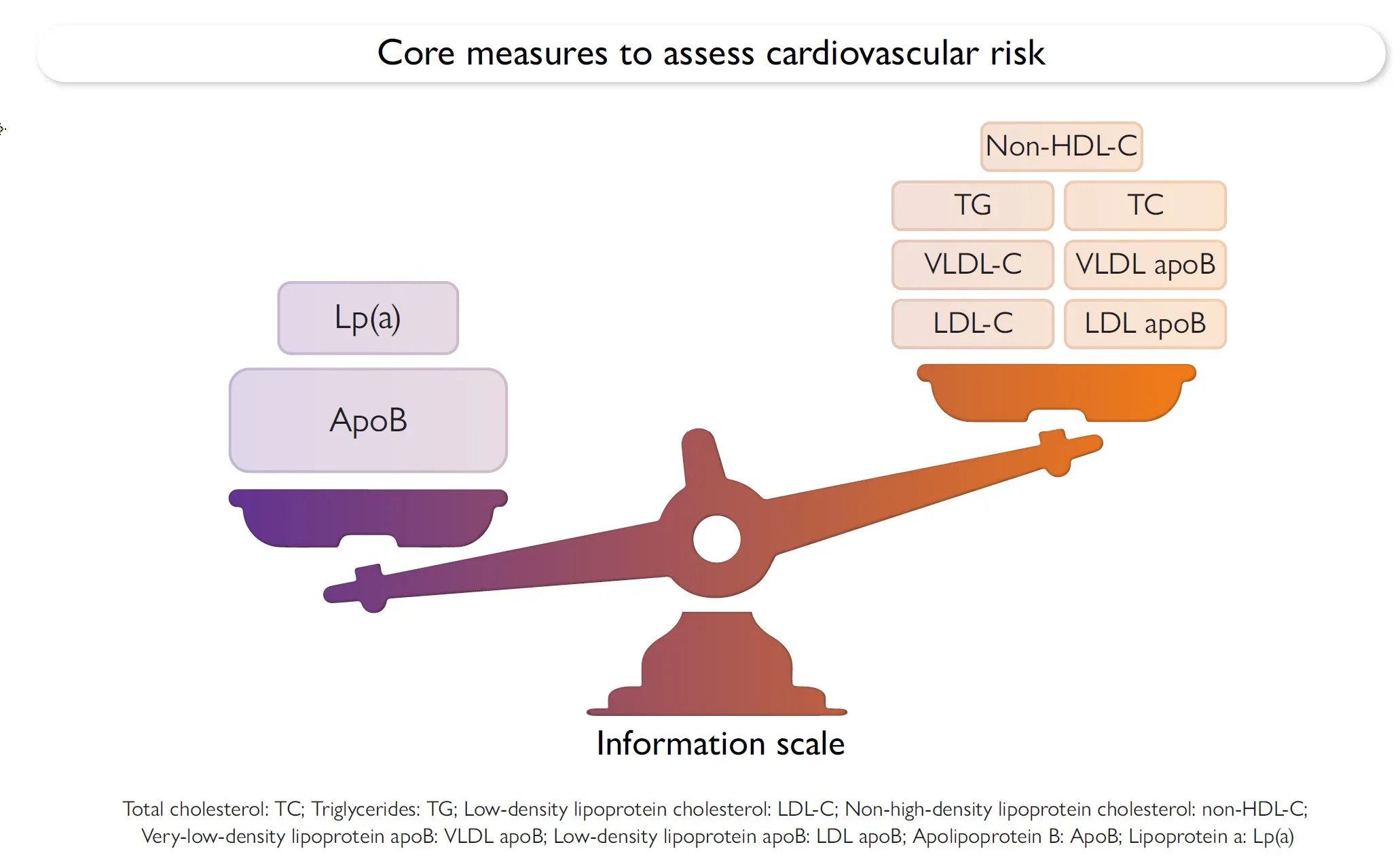 ApoB and Lp(a) are more accurate than cholesterol, triglycerides, and particle sizes. Source: European Heart Journal, 2025
ApoB and Lp(a) are more accurate than cholesterol, triglycerides, and particle sizes. Source: European Heart Journal, 2025
In this post, we’ll explain three specific reasons why ApoB is better, the evidence we use to compare two different biomarkers, and then a quick guide to the other independent risk factors for heart disease (so that you have a complete picture).
ApoB vs LDL cholesterol: why is ApoB more accurate?
ApoB is more accurate than LDL cholesterol for three reasons: ApoB is always measured (rather than calculated), ApoB counts every atherogenic particle (including IDL and VLDL), and ApoB counts the number of particles rather than their mass. Let’s go through each reason one by one.
LDL is sometimes calculated; ApoB is always measured
LDL-C is often calculated from total cholesterol, HDL cholesterol, and triglycerides, rather than measured directly. A common approximation is the Friedewald equation:
LDL-C = Total Cholesterol - HDL-C - (Triglycerides / 5)
This equation is less accurate when triglycerides are high. Newer equations, like Sampson’s equation or the Martin-Hopkins formula, close part of that gap. But even the best modern formula still misses about a sixth of what ApoB captures. We tested this on our own data in do modern LDL formulas replace ApoB?.
LDL is just one of three atherogenic particles. ApoB counts all of them.
The particles in your blood that cause heart disease are called lipoproteins, and they come in many sizes and densities. Each lipoprotein contains about 3,000-6,000 fat molecules, which are a mix of cholesterol and triglycerides. The density of the lipoprotein is the main factor that determines whether it’s atherogenic (i.e., causes heart disease). VLDL (very low density lipoprotein), LDL (low density lipoprotein), and IDL (intermediate density lipoprotein) are three different particle types that cause heart disease. HDL (high density lipoprotein) doesn’t get heart disease, and may even protect against it.
VLDL, LDL, and IDL particles each contain exactly one ApoB molecule, as shown in this diagram:
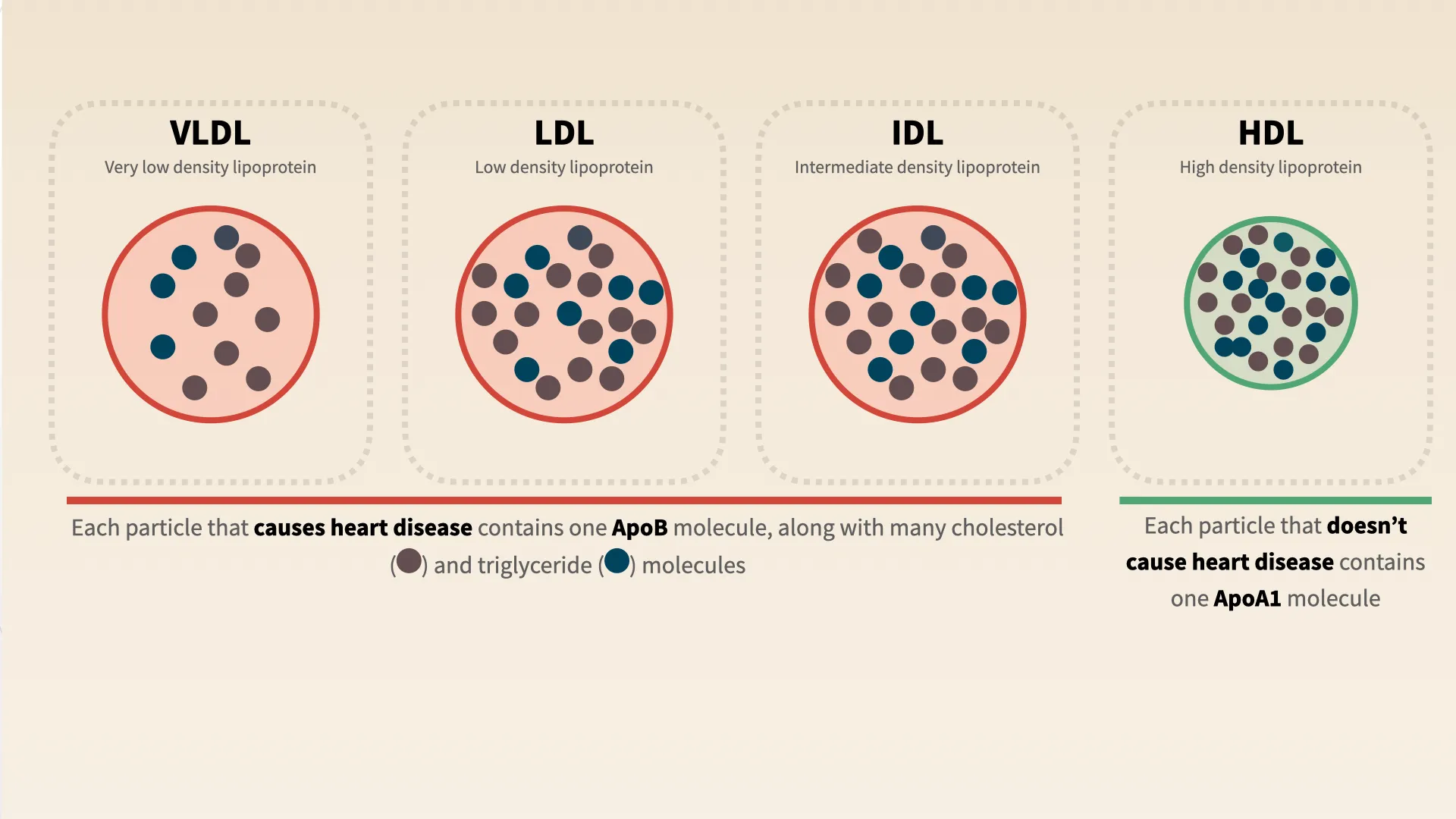 Every cholesterol particle that causes heart disease contains one ApoB molecule
Every cholesterol particle that causes heart disease contains one ApoB molecule
ApoB (apolipoprotein B) is a protein found on the surface of all atherogenic lipoproteins. Critically, each particle that causes heart disease contains exactly one ApoB molecule.
This means that if your LDL is normal, but your IDL or VLDL are high, ApoB will catch your risk of heart disease. This is part of why about 20% of people with normal LDL will have elevated ApoB, and be at risk of heart disease.
LDL counts mass, whereas ApoB counts number of particles
When you receive an LDL number from a blood test (typically in mg/dL), it’s telling you the total mass within the LDL particle. But research studies show that the number of these particles is a stronger driver of plaque buildup and heart attack risk than the total cholesterol they contain. Even if LDL-C is normal, a high number of cholesterol-poor LDL particles (reflected by high ApoB) can still increase risk.
Dr. Michael Shapiro at Wake Forest uses a traffic analogy: “a standard lipid panel is similar to counting the number of passengers on the road. ApoB is like counting the number of cars.” What causes traffic, too many passengers or too many cars? It’s the cars, and that’s ApoB.
ApoB vs LDL-C: what happens in discordance
A comprehensive 2025 review in the European Heart Journal (Sniderman et al.) summarizes decades of research:
- ApoB is a more accurate predictor of cardiovascular events than LDL-C or non-HDL cholesterol.
- Discordance between ApoB and LDL-C is common, especially in people with metabolic syndrome, diabetes, or high triglycerides.
- When ApoB and LDL-C disagree, ApoB is the better predictor of risk.
The CARDIA study found that young adults with high ApoB but normal LDL-C had a 55% higher risk of developing coronary artery calcification (a marker of plaque) 25 years later, while those with high LDL-C but normal ApoB did not show increased risk.
Guidelines on ApoB vs LDL are changing
The European Society of Cardiology and Canadian Cardiovascular Society have recommended ApoB over LDL-C for risk assessment and treatment targets since 2019 and 2021, respectively. In March 2026, the U.S. caught up: the 2026 AHA/ACC dyslipidemia guidelines now formally recommend ApoB measurement (COR 2a) for adults on lipid-lowering therapy — particularly those with ASCVD, cardiovascular-kidney-metabolic syndrome, type 2 diabetes, or elevated triglycerides — to guide treatment decisions once LDL-C and non-HDL-C goals are achieved. Despite this, less than 1% of insured Americans get ApoB measured each year.

Is ApoB the only cardiovascular risk factor you need?
No. ApoB can be thought of as a more accurate LDL. But to assess your overall risk of heart disease, you also need to understand blood pressure, inflammation (hs-CRP), Lp(a), HbA1c, and eGFR (kidney health). Each of these are independent risk factors, so by knowing all of them, you can most accurately measure and reduce your risk of heart disease.
To learn what your ApoB and LDL targets should be, see normal cholesterol levels. To reduce your ApoB through diet and lifestyle, the most effective interventions are increasing soluble fiber and reducing saturated fat. For a full guide, see how to lower your ApoB.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
