Why more young adults are dying of heart attacks
Heart attacks have traditionally been considered an older person’s disease. That assumption is increasingly wrong.
A new study in the Journal of the American Heart Association analyzed nearly 1 million hospitalizations of U.S. adults ages 18–54 from 2011-2022. The study found the number of adults ages 18-54 who died of a severe first heart attack rose 57% between 2011 and 2022. Women fared worse than men, with 3.1% mortality vs. 2.6% in men for severe heart attacks.
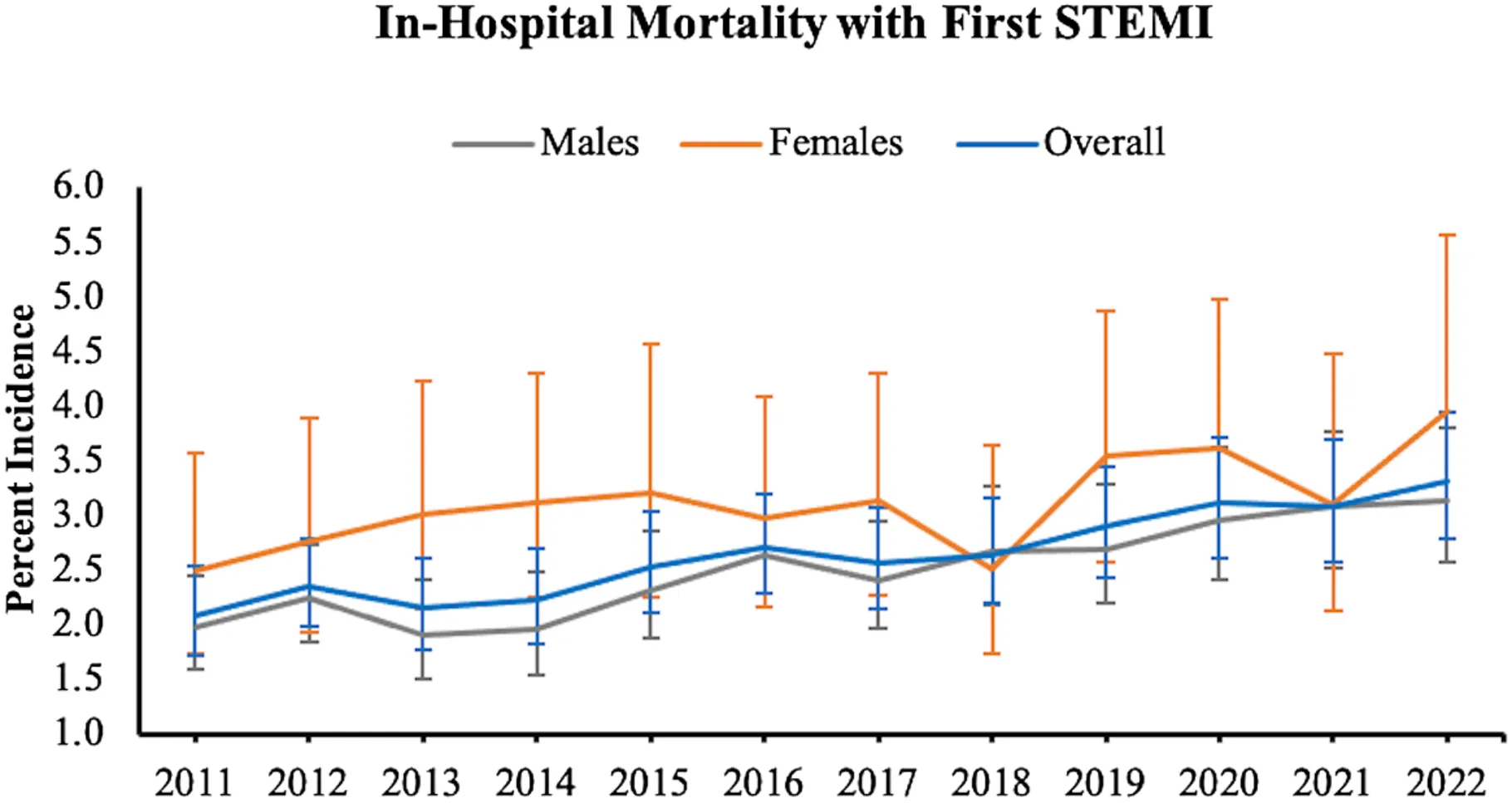 Heart attack deaths in young people are rising (Source: Journal of the American Heart Association)
Heart attack deaths in young people are rising (Source: Journal of the American Heart Association)
One in five heart attacks now occurs in someone under 40, double the rate from a decade ago.
The reasons that more young adults are dying of heart attacks include obesity, COVID-19, vaping, poverty, primary care access, inflammation, and microplastics. We’ll go through each cause one by one.
“We often think heart attacks are mainly an older person’s problem; however, our findings indicate that younger adults, especially women, are at real risk.”
— Dr. Mohan Satish, lead study author
Obesity is rising among young adults
Between 2009 and 2020, obesity rates in young adults rose from 32.7% to 40.9%. Nearly half of adults aged 20–44 now have at least one major cardiovascular risk factor. Deaths from obesity-related ischemic heart disease increased 180% from 1999 to 2020.
The key driver is duration of exposure to obesity. A 35-year-old who has been obese since age 15 carries far more cardiovascular risk than their current BMI alone suggests. Twenty years of insulin resistance, chronic inflammation, and endothelial dysfunction accelerate atherosclerosis in arteries that should still be young.
The AHA recognized this in 2023 by defining Cardiovascular-Kidney-Metabolic (CKM) Syndrome. CKM is a framework that treats obesity, diabetes, kidney disease, and heart disease as a single interconnected condition rather than separate problems.
COVID-19 accelerated heart disease risk in young people
COVID didn’t start the trend, but it made it worse. A Cleveland Clinic / USC study using UK Biobank data found that heart attack, stroke, and death risk was 2x higher among all COVID patients and 4x higher among those hospitalized. Elevated heart disease risk from COVID-19 persisted for up to three years after infection.
The mechanisms are well-documented: viral persistence in heart tissue, chronic arterial inflammation, endothelial dysfunction, and a pro-thrombotic state. During the first year of the pandemic, COVID patients had a 16x risk of myocarditis compared to non-COVID patients. Across 16 countries, excess cardiovascular deaths totaled an estimated 742,000 in 2020 alone.
Cannabis, stimulants, and vaping are underappreciated cardiac risks
The AHA study flagged non-tobacco drug use as a stronger predictor of in-hospital death than high cholesterol. The research backs this up:
- Cannabis: The largest pooled analysis to date (ACC.25, March 2025) studied 4.6 million people and found cannabis users under 50 had a 6x increased risk of heart attack, even among those with no baseline cardiovascular comorbidities, normal blood pressure, normal LDL, and no tobacco use.
- Cocaine and methamphetamine: Users were 2.5–3x more likely to have premature heart disease. Polysubstance use (4+ substances) was associated with a 9-fold increase.
- Vaping: A 2025 systematic review found that even nicotine-free e-cigarettes caused acute vascular impairments including endothelial dysfunction, oxidative stress, and increased arterial stiffness.
Poverty and stress
The AHA study found low income was more predictive of death than traditional risk factors like cholesterol or blood pressure. This is consistent with a UCSF study that estimated 60–70% of excess heart disease among low-income Americans is attributable to poverty itself. The biological pathway is becoming clearer. An NIH study found that people in the lowest-income neighborhoods had higher stress-related amygdala activity and a 4x risk of a major cardiac event over 5 years. While evidence is still developing, this brain-inflammation pathway may account for 28% of poverty’s total effect on heart disease.
Young adults aren’t getting screened for cardiac risk factors due to a primary care shortage
One in five U.S. young adults has hypertension, but awareness has declined since 2013–2014. Among 18–39 year-olds, hypertension awareness is only 27% compared to 74% for those over 60. The numbers for other conditions are similar: 2 in 5 young adults with diabetes don’t know they have it, 1 in 4 with high cholesterol don’t know they have it. This is the effect of a major primary care shortage. It now takes months to get a primary care appointment.
Environmental exposures like microplastics, ultra-processed food, air pollution
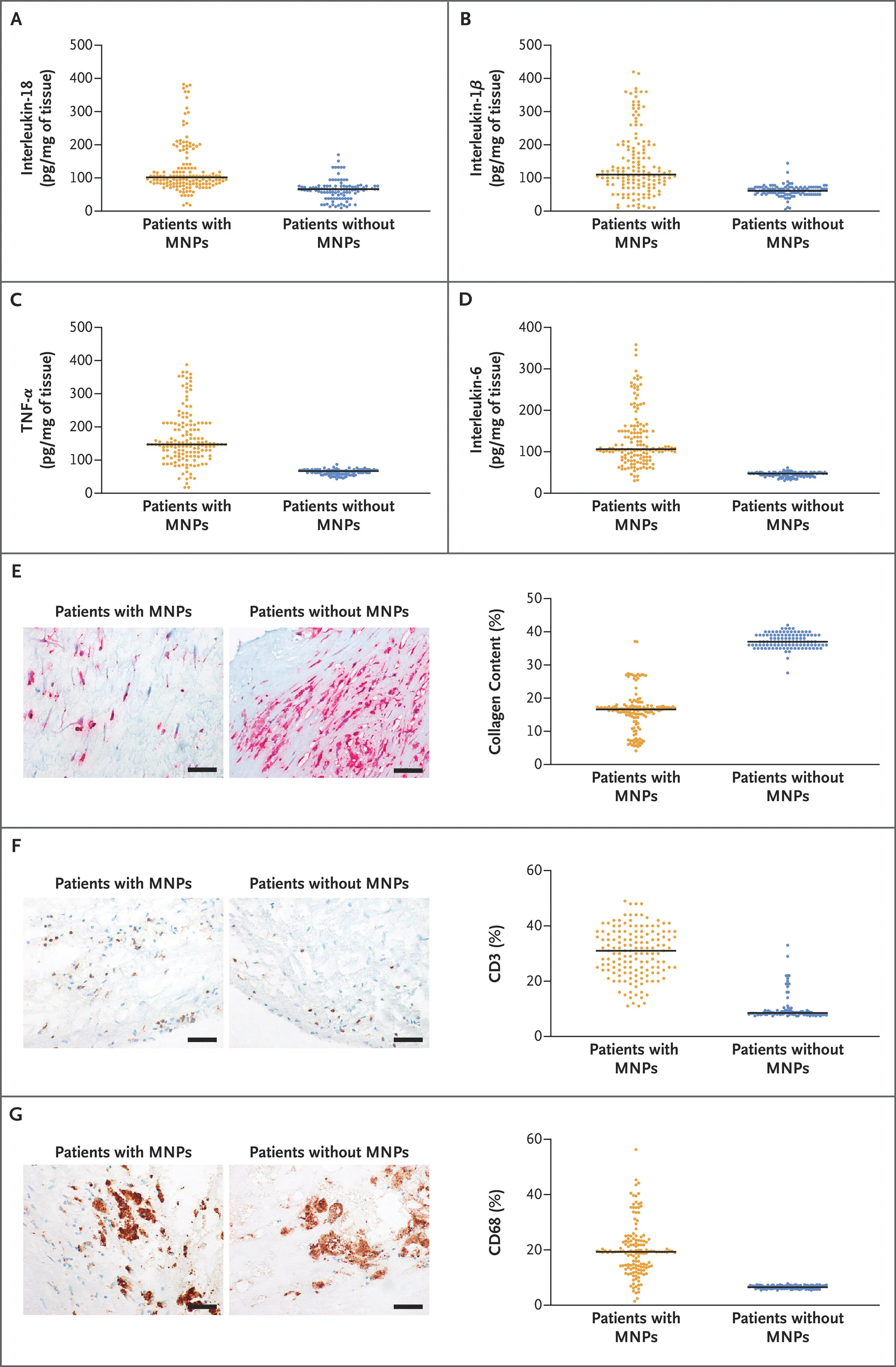 Inflammatory markers in plaque samples (Source: NEJM)
Inflammatory markers in plaque samples (Source: NEJM)
Emerging research points to environmental contributors that affect everyone, not just high-risk groups. A landmark 2024 NEJM study found microplastics in 58% of carotid artery plaques. Patients with detectable microplastics had a 4.5x higher risk of heart attack, stroke, or death over 34 months. A UC Riverside study (2025) showed microplastics accelerated atherosclerosis in mice without raising cholesterol, suggesting a direct inflammatory mechanism. Ultra-processed foods have also been linked to cardiovascular mortality, with 10–14% of premature deaths in the U.S. attributable to ultra-processed food consumption. Finally, each 10 μg/m³ increase in air pollution (PM2.5) was associated with a 43% increase in fatal coronary heart disease.
Heart disease in young people has several causes
The metabolic deterioration of young adults has been building for 20 years. COVID layered acute vascular damage on top. Cannabis legalization and vaping introduced new cardiovascular stressors into a generation that simultaneously avoids preventive care, lives under financial stress, eats more ultra-processed food, and carries a higher microplastics burden than any prior generation. Te healthcare system isn’t designed to catch any of this before a cardiac event.
What you can do to reduce your heart attack risk
The AHA study’s most actionable finding may be that the strongest predictors of death (kidney disease, metabolic dysfunction, ApoB, inflammation) are detectable with a blood test. You don’t need to wait for chest pain. New markers like ApoB, Lp(a), hs-CRP, HbA1c, and kidney function (GFR, creatinine) paint a much more complete picture. An advanced heart panel covers all of these. Kidney function and inflammatory markers matter as much, or more, than LDL cholesterol alone.
Don’t assume you’re too young. If you have a family history, carry excess weight, use cannabis or stimulants, or simply haven’t had bloodwork in years, the data says you’re not too young to be at risk.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
