Lp(a) testing is up 22x in the last decade. It's now recommended for everyone.
Ten years ago, Lp(a) was an obscure protein only known to lipidologists. In the last decade, Lp(a) testing has grown 22x and the AHA now recommends everyone test Lp(a) at least once. (This recommendation is new in the American Heart Association and American College of Cardiology’s 2026 guidelines)
Yet, only 0.24% of people are testing their Lp(a) today. In this post, we’ll explain what Lp(a) is, why it’s the strongest inherited risk factor for heart disease, and how the guidelines changed in 2026, and how to test your Lp(a).
Briefly, what is Lp(a)?
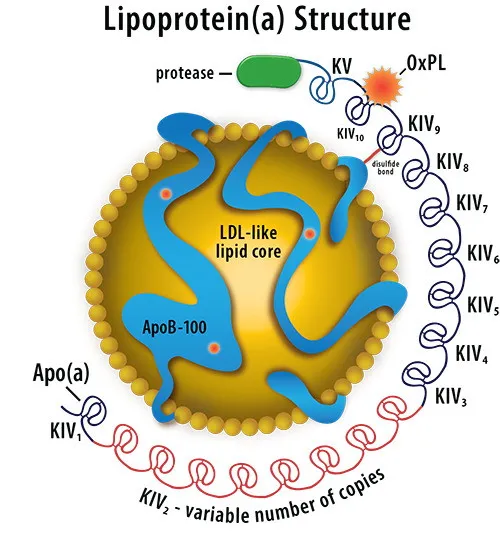 Each Lp(a) particle has an LDL cholesterol core, an ApoB structural protein, and an apoprotein (a) protein wrapping the whole structure. Details in our post on the science of Lipoprotein(a)
Each Lp(a) particle has an LDL cholesterol core, an ApoB structural protein, and an apoprotein (a) protein wrapping the whole structure. Details in our post on the science of Lipoprotein(a)
Each Lp(a) particle is a cholesterol particle with an extra protein wrapped around it. The extra protein camoflauges it from your liver, making it about 6.6x more atherogenic than ordinary cholesterol. We wrote more about the science of Lipoprotein(a) describes in more detail. For those post, we’ll focus on trends in testing.
Only 1 in 400 people test their Lp(a)
Researchers at UCSD analyzed of 300 million patient records. Only 1 in 400 people have taken an Lp(a) blood test even though the AHA recommends it for everyone.
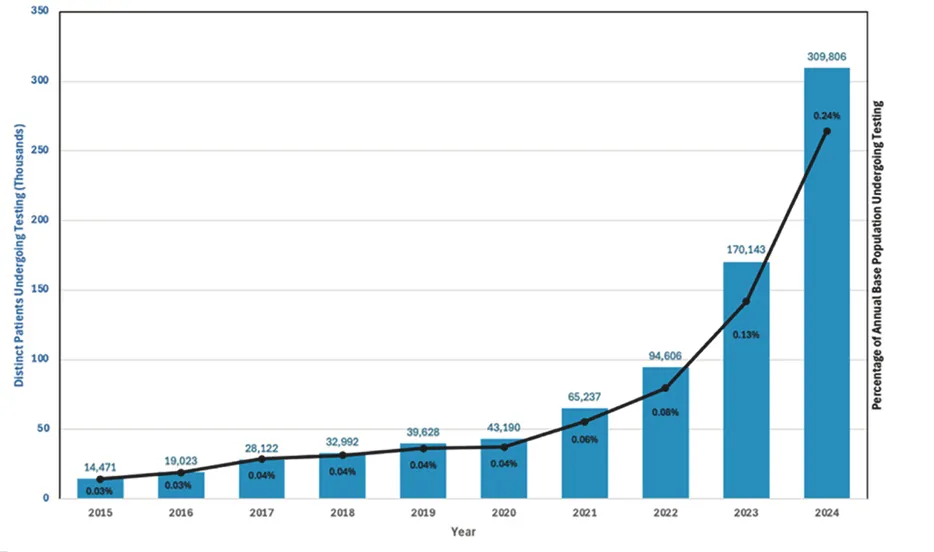 Testing of Lp(a) has increased by 22x in the last decade, but is still only 1 in 400 people. Source: Journal of the American College of Cardiology, 2025
Testing of Lp(a) has increased by 22x in the last decade, but is still only 1 in 400 people. Source: Journal of the American College of Cardiology, 2025
However, testing of Lp(a) has increased substantially over the last decade.
The AHA/ACA now recommend Lp(a) testing for all
In Mar 2026, the American Heart Association and American College of Cardiology started recommending that everyone test for Lp(a). This is a major shift in the guidelines. The previous 2018 guidelines mentioned Lp(a) only as a “risk enhancer” without a specific testing recommendation. The new 2026 dyslipidemia guidelines gave Lp(a) testing a class 1 recommendation, the strongest they issue.
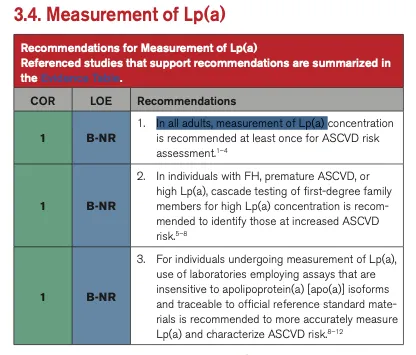 The 2026 guidelines now recommend universal testing of Lipoprotein(a). Source: 2026 ACC/AHA Dyslipidemia Guideline.
The 2026 guidelines now recommend universal testing of Lipoprotein(a). Source: 2026 ACC/AHA Dyslipidemia Guideline.
What counts as elevated Lp(a)?
About 20% of people have elevated Lp(a) levels (≥125 nmol/L or ≥50 mg/dL). At that threshold, ASCVD risk increases by about 40%. At very high levels (≥250 nmol/L), risk doubles.
| Lp(a) level | Relative ASCVD risk increase |
|---|---|
| <75 nmol/L (<30 mg/dL) | Reference (low) |
| 75–124 nmol/L (30–49 mg/dL) | 1.2× |
| ≥125 nmol/L (≥50 mg/dL) | 1.4× |
| ≥250 nmol/L (≥100 mg/dL) | 2× |
| ≥350 nmol/L (≥150 mg/dL) | 3× |
| ≥430 nmol/L (≥180 mg/dL) | 4× |
Data from the UK Biobank Study, as cited in the 2026 AHA/ACC guideline.
What to do if your Lp(a) is elevated
There are no FDA-approved drugs specifically for lowering Lp(a) yet. Four Lp(a) drugs are in clinical trials: lepodisiran (Eli Lilly) lowered Lp(a) by 93.9% in a Phase II trial, and pelacarsen (Novartis) results from the Lp(a) HORIZON trial are expected this year.
In the meantime, the guidelines recommend aggressive ApoB management, PCSK9 inhibitors (for some), and cascade testing (if your Lp(a) is elevated, your parents, siblings, and children should be tested too).
How to get your Lp(a) tested
If you haven’t had your Lp(a) measured, the AHA/ACC now says you should. Empirical’s comprehensive heart panel includes Lp(a), ApoB, hsCRP, and the other biomarkers emphasized in the new guidelines, available direct to you starting at $190.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
