“Saturated fat raises cholesterol.” You’ve heard it a thousand times. While a useful heuristic, the science is actually much more specific. Three saturated fatty acids—Lauric (12:0), myristic (14:0), and palmitic (16:0)—drive most of the change in LDL cholesterol (or ApoB).
This explains why dark chocolate (rich in stearic acid) is good for the heart, whereas coconut oil isn’t. It also explains why some fatty foods, like avocados (palmitic acid, majority oleic acid, lots of fiber).
In this post, I’ll review the science of saturated fat (from controlled feeding trials and mechanistic evidence), break down specific foods in terms of their saturated fatty acid composition, and then summarize the most practical things to actually do in your day to day life.
 Saturated fat interacts with fiber to drive cardiovascular mortality. While this article focuses on the science of saturated fatty acids, saturated fat is
one part of a more comprehensive comprehensive approach to data-driven nutrition.
Saturated fat interacts with fiber to drive cardiovascular mortality. While this article focuses on the science of saturated fatty acids, saturated fat is
one part of a more comprehensive comprehensive approach to data-driven nutrition.
Three saturated fats matter: lauric, myristic, and palmitic acid
Lauric, myristic, and palmitic acids acids are the primary drivers of LDL cholesterol:
| Fatty acid | Carbon chain | Relative potency | Primary food sources |
|---|---|---|---|
| Lauric acid (C12:0) | 12 carbons | Moderate | Coconut oil, palm kernel oil |
| Myristic acid (C14:0) | 14 carbons | Highest per gram | Dairy fat, coconut oil, nutmeg |
| Palmitic acid (C16:0) | 16 carbons | Moderate, but highest total impact | Palm oil, meat, dairy, most foods |
By the gram, myristic acid is the most potent cholesterol-raiser. In a head-to-head trial by Zock et al. (1994), a myristic acid-enriched diet produced mean serum cholesterol of 5.19 mmol/L versus 4.96 mmol/L for palmitic acid . But palmitic acid is the biggest contributor to population-level LDL elevation for a simple reason: we eat far more of it. Palmitic acid accounts for roughly 55–60% of total saturated fat intake in Western diets (about 20–30 g per day). It’s the most common saturated fatty acid in meat, dairy, and palm oil.
Lauric acid is an interesting case. It raises total cholesterol substantially, but a large portion of its effect is on HDL rather than LDL. This means lauric acid actually improves the total-to-HDL cholesterol ratio, complicating simple risk assessments. Still, it reliably raises LDL, and LDL remains the primary causal factor in atherosclerosis.
The science: controlled feeding studies of saturated fats.
Even the earliest studies on how diet affects cholesterol noted that not all saturated fats are created equal.
In 1965, Mark Hegsted and Ancel Keys independently derived equations predicting how dietary fats affect serum cholesterol from metabolic ward studies. Both recognized early on that not all saturated fats behave the same. Keys explicitly noted that stearic acid and saturated fatty acids with fewer than 12 carbons have “negligible effects” on serum cholesterol.
In 1993, Ronald Mensink published a focused review in the American Journal of Clinical Nutrition examining how individual saturated fatty acids differ in their effects on serum lipids. This 1993 paper laid the groundwork for everything that followed, establishing the core thesis: “saturated fatty acids are not all equally hypercholesterolemic: stearic acid (18:0) and saturated fatty acids with < 12 carbon atoms are thought not to raise serum cholesterol concentrations.”
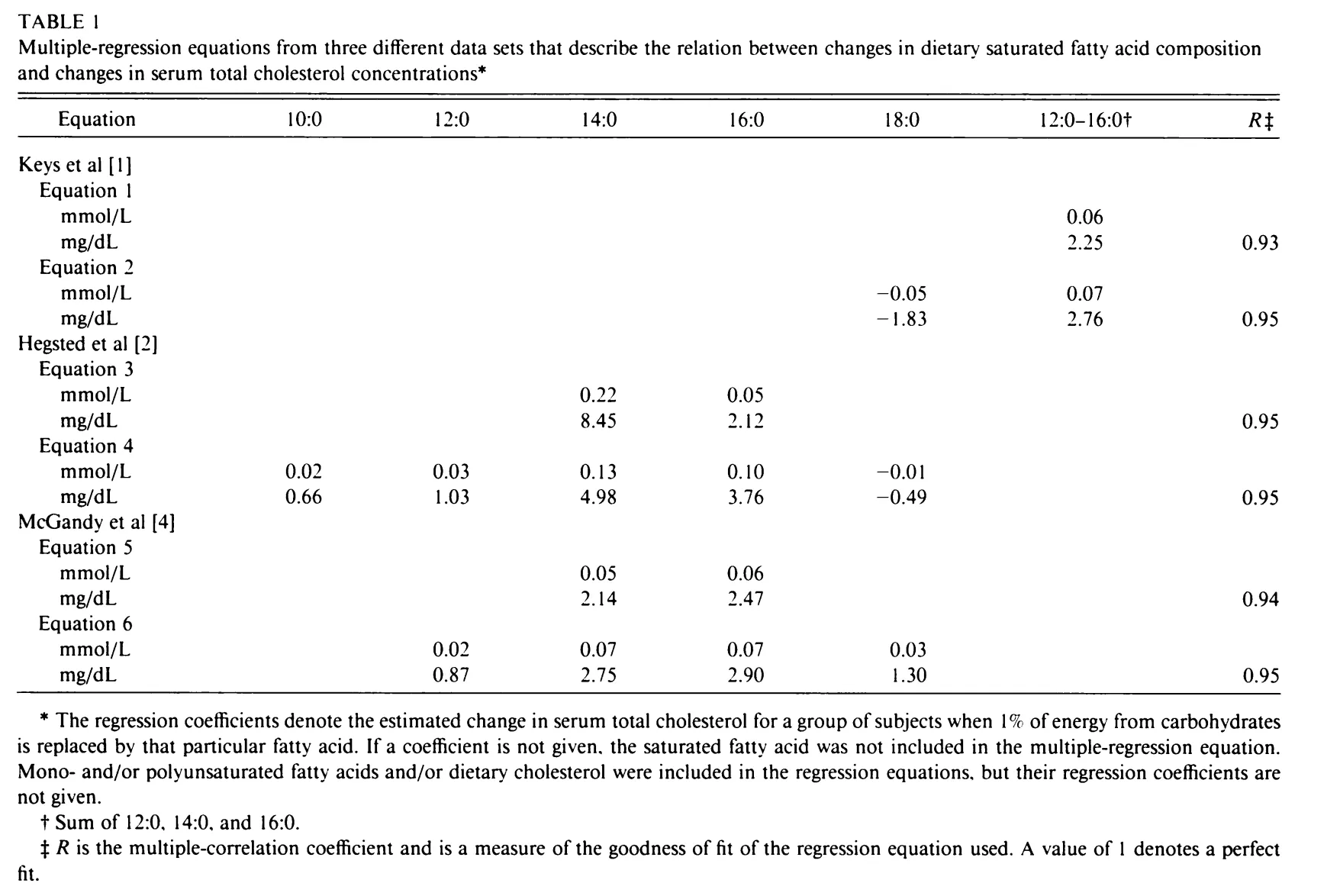 Serum cholesterol concentration vs. individual saturated fatty acids. Source: (American Journal of Clinical Nutrition)[https://pubmed.ncbi.nlm.nih.gov/8475888/]
Serum cholesterol concentration vs. individual saturated fatty acids. Source: (American Journal of Clinical Nutrition)[https://pubmed.ncbi.nlm.nih.gov/8475888/]
Mensink showed that while lauric, myristic, and palmitic acid all raised serum cholesterol, their potencies differed, with myristic acid appearing more potent than palmitic, and lauric acid’s effect being somewhat weaker. The definitive analysis came 10 years later, in Mensink’s 2003 meta-analysis of 60 controlled dietary trials. By pooling data across thousands of participants, Mensink quantified the effect of each individual fatty acid on blood lipids when substituted for carbohydrates. Lauric, myristic, and palmitic acid all significantly raised LDL cholesterol. Stearic acid (C18:0) had no significant effect on LDL. All three cholesterol-raising fatty acids also raised HDL, with lauric acid having the strongest HDL-raising effect. This analysis provided the clearest evidence that the cholesterol-raising effect of “saturated fat” is really the effect of three specific molecules.
The American Heart Association’s 2017 advisory by Sacks et al. reviewed the full body of evidence from randomized controlled trials and concluded that replacing saturated fat with polyunsaturated fat reduced cardiovascular events by approximately 30% (an effect size comparable to statins).
How your liver processes these three saturated fats
We have some mechanistic evidence that centers centers on a liver enzyme called ACAT (acyl-CoA:cholesterol acyltransferase). ACAT packages free cholesterol for storage by esterifying it.
Saturated fatty acids are poor substrates for ACAT compared to unsaturated fatty acids. Palmitic, myristic, or lauric acid arrive at the liver but can’t efficiently feed the ACAT reaction. Then free (unesterified) cholesterol accumulates inside liver cells. The buildup suppresses SREBP-2, a transcription factor that controls LDL receptor production. With fewer LDL receptors on liver cell surfaces, less LDL is cleared from the bloodstream, causing blood LDL cholesterol to rise.
Unsaturated fatty acids do the opposite: they’re excellent ACAT substrates, which keeps free cholesterol low, SREBP-2 active, LDL receptors plentiful, and blood LDL low.
This mechanism has been validated in hamster models showing dose-dependent reductions in LDL receptor mRNA with myristic and palmitic acid feeding, in primate studies showing LDL receptor downregulation from all three fatty acids, and in human studies showing that reducing dietary saturated fat increases LDL receptor number proportionally to the decrease in serum LDL.
Some saturated fatty acids that don’t raise cholesterol
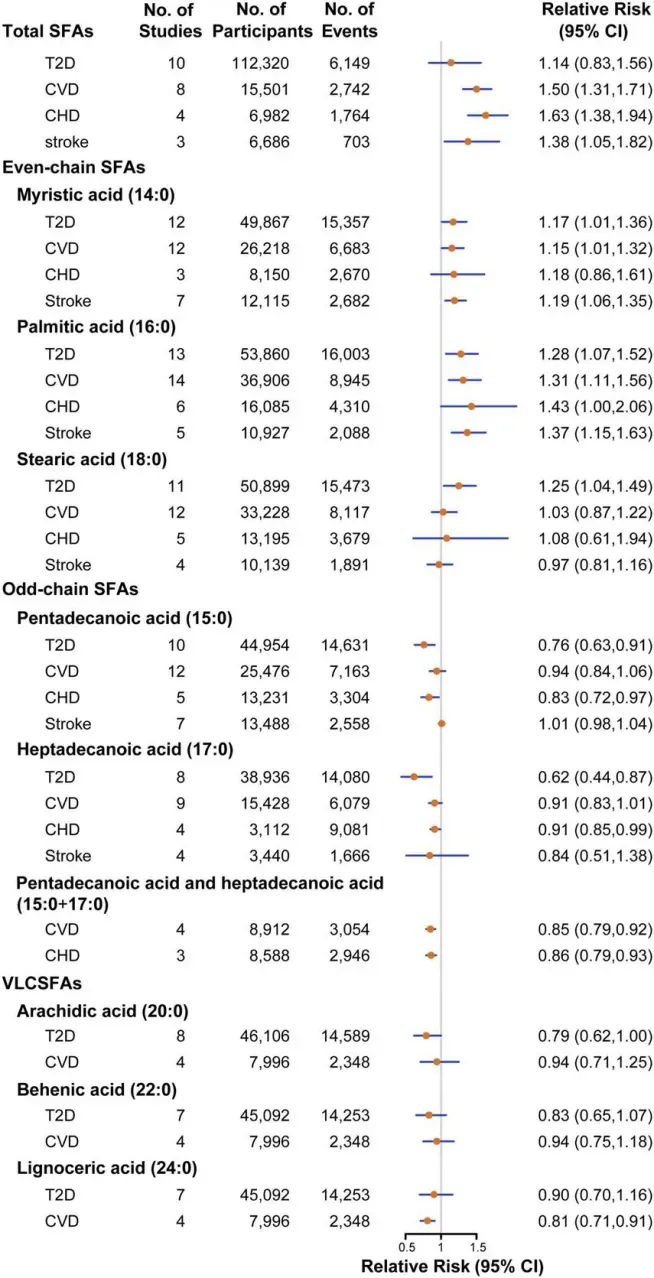 Meta analysis of saturated fatty acids and heart disease source
Meta analysis of saturated fatty acids and heart disease source
Stearic acid (C18:0) (dark chocolate)
Stearic acid is an 18-carbon saturated fat found abundantly in cocoa butter, beef fat, and shea butter. Despite being fully saturated, it has a neutral effect on LDL cholesterol. The reason is that the liver rapidly converts stearic acid to oleic acid (a monounsaturated fat) via the enzyme stearoyl-CoA desaturase. Stearic acid is so insoluble that it gets desaturated before it can influence cholesterol metabolism. This means that metabolically, eating stearic acid is similar to eating olive oil.
This is why dark chocolate (cocoa butter is roughly one-third stearic acid) consistently shows neutral or favorable effects on blood lipids in clinical trials.
Short- and medium-chain fatty acids (C4–C10)
Saturated fatty acids with fewer than 12 carbons — butyric acid (C4) in butter, caprylic acid (C8) and capric acid (C10) in coconut and MCT oil — follow a different metabolic route entirely. They’re absorbed directly into the portal vein rather than being packaged into chylomicrons, bypassing the lipoprotein pathway. Keys recognized in 1965 that these short-chain fats have negligible effects on cholesterol, and subsequent research has confirmed this. A 2023 systematic review in Nutrients found short- and medium-chain saturated fats showed a neutral to potentially beneficial association with cardiovascular risk.
What you replace saturated fat with matters enormously
So far, we’ve nerded out on the science. But one of the most important implications of this science is that cutting saturated fat only helps if you replace it with something better. Here are your options:
- Replacing saturated fat with polyunsaturated fat (PUFA) produces clear cardiovascular benefit. A pooled analysis of randomized trials estimated roughly a 10% reduction in CVD risk for every 5% of energy shifted from saturated fat to polyunsaturated fat. This aligns closely with the predicted LDL reduction.
- Replacing saturated fat with monounsaturated fat (MUFA) — think olive oil, avocados, nuts — also lowers LDL effectively, though fewer randomized trial data exist for hard cardiovascular endpoints.
- Replacing saturated fat with refined carbohydrates is not helpful.. LDL decreases, but triglycerides rise, HDL falls, and the net effect on cardiovascular events is approximately zero. This is the substitution that confused a generation of nutrition science: when the low-fat movement of the 1980s and ’90s replaced butter with white bread and sugar, heart disease didn’t budge.
- Replacing saturated fat with whole grains or plant protein is beneficial. A 2016 Harvard analysis found that replacing 1% of calories from palmitic acid with plant proteins or polyunsaturated fat was associated with an 11–12% reduction in coronary heart disease risk.
What about oxidation and inflammation?
The three fatty acids raise ApoB, but ApoB is only one of six cardiovascular risk factors. In the discussion section of his 1993 review, Mensink raised a point that remains relevant today — the role of antioxidants in modifying how dangerous those LDL particles actually are:
“Antioxidants like vitamin E, I think, have no effect on these concentrations but they may reduce the atherogenicity of lipoproteins, and of the LDL particles in particular, by preventing their oxidative modification and subsequent uptake by macrophages.”
In other words, even if your LDL is elevated, the degree to which those particles get oxidized (and subsequently engulfed by immune cells in artery walls) matters for whether atherosclerosis actually progresses. Vitamin E and other antioxidants don’t change how much LDL is in your blood, but they may change how much damage it does once it’s there. The American College of Cardiology now recommends that everybody measure inflammation (hs-CRP) for heart health.
Coconut oil is surprisingly unhealthy
Coconut oil deserves special mention because it delivers all three cholesterol-raising saturated fatty acids simultaneously: approximately 50% lauric acid, 18% myristic acid, and 8% palmitic acid. A 2020 meta-analysis in Circulation confirmed that coconut oil significantly raises LDL cholesterol compared to nontropical vegetable oils.
The common claim that coconut oil is “healthy” because it raises HDL doesn’t hold up under scrutiny. While coconut oil does increase HDL, raising HDL pharmacologically has not been shown to reduce cardiovascular events. (This finding has been replicated by multiple failed HDL-raising drug trials). The ApoB/LDL increase is the more important signal.
TL;DR: saturated fat, cholesterol, & heart health
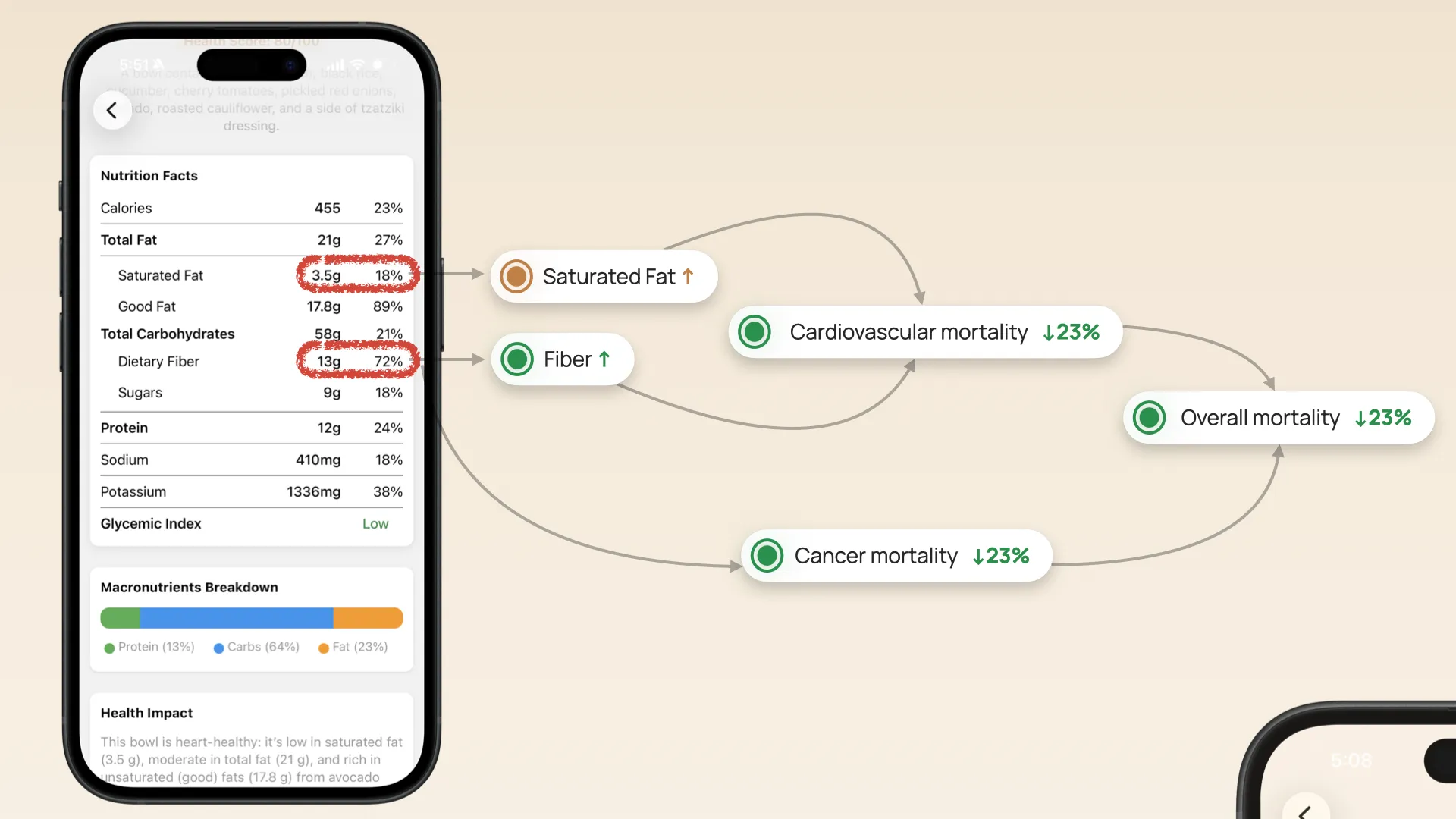
![]() Tracking saturated fat with Empirical Health. These are tracked as density per calorie, as well as the ratio of fiber to saturated fat.
Tracking saturated fat with Empirical Health. These are tracked as density per calorie, as well as the ratio of fiber to saturated fat.
The “saturated fat and cholesterol” story is more nuanced than either side of the debate typically acknowledges. Three specific saturated fatty acids drive heart disease. If you just want to know what to do to reduce your risk of heart disease, do this:
- Reduce palmitic & myristic acid — less palm oil, less fatty meat, less coconut oil, less full-fat dairy.
- Be strategic about lauric acid — primarily from coconut oil. Its HDL-raising effect is real but doesn’t offset the LDL increase.
- *Track rigorously - nowadays, apps like Empirical Health let you track saturated fat with just a food photo.
- Don’t worry about stearic acid — dark chocolate and cocoa butter are not in the same risk category.
- Replace with unsaturated fats, not refined carbs — this is the single most important nuance in the entire field.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
