Updated Mar 2026 to reflect the AHA/ACC’s new 2026 guidelines
If every person reduced their ApoB to 20-30 mg/dL in their 20s, heart disease would be eliminated.
The statement is hyperbolic, but shows how the approach to lipid management is changing. In 2019, the European Society of Cardiology concluded that ApoB is a more accurate marker of cardiovascular risk than LDL cholesterol. In 2021, the Canadian Cardiovascular Society recommended ApoB over LDL-C as the primary metric for lipid management. ApoB has become the gold standard of cardiovascular risk.
In March 2026, the U.S. caught up: the 2026 AHA/ACC dyslipidemia guidelines now formally recommend ApoB measurement for adults on lipid-lowering therapy, particularly those with ASCVD, cardiovascular-kidney-metabolic syndrome, diabetes, or elevated triglycerides. Despite this, less than 1% of the insured population gets their ApoB tested each year.
The rest of this post will explain why ApoB is more accurate than LDL cholesterol, why getting more people tested can help save lives, normal ranges, insurance coverage, and cash pay options.
What are lipoproteins? Why is ApoB atherogenic?
Lipoproteins are molecules in your blood made of fats (e.g. cholesterol, triglycerides) and proteins. They’re critical for many physiological processes, like hormone production, bile acid synthesis, and cell membrane formation.
However, at excess quantities, some lipoproteins are atherogenic—meaning they can enter your arterial walls, form plaques, and cause heart attacks.
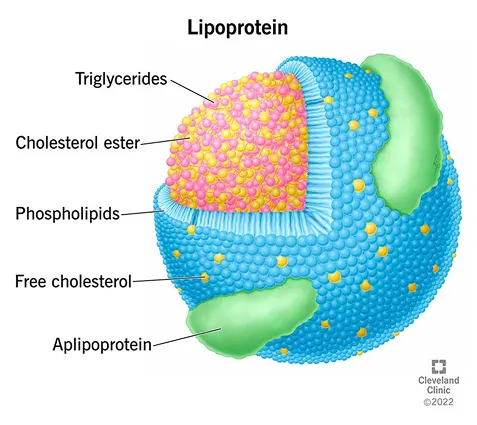
A lipoprotein. Source: Cleveland Clinic
Which lipoproteins contain ApoB (and increase cardiovascular risk)
ApoB stands for Apolipoprotein B.
An apolipoprotein is the green blob in the image above. It’s a protein wrapper around a lipoprotein that helps make it soluble in plasma, maintains its structure, and helps with binding during tissue uptake.
There are four main atherogenic lipoproteins:
| Lipoprotein | Function | Size |
|---|---|---|
| vLDL: Very Low-Density Lipoprotein | Triglyceride transport | Large |
| IDL: Intermediate-Density Lipoprotein | Intermediate LDL precursor | Medium |
| LDL: Low-Density Lipoprotein | Deliver cholesterol to cells | Small |
| Lipoprotein(a) | Deliver cholesterol to cells | Small |
What is the ApoB blood test?
An ApoB blood test measures the concentration of apolipoprotein B (ApoB) in your blood. Since each atherogenic lipoprotein particle carries exactly one ApoB molecule, the test is a good indicator of the total number of atherogenic particles—and thus your cardiovascular risk.
Lipid panels vs ApoB
A standard lipid panel in the U.S. includes:
- Total cholesterol
- HDL
- Triglycerides
- LDL-C
- Cholesterol/HDLC Ratio
- LDL/HDL Ratio
- Non HDL Cholesterol
You’ll notice it doesn’t include ApoB. One reason for this is increased cost vs. other countries, but the end result is that treatment for high cholesterol is mostly based on LDL-C in the U.S.
As mentioned in a previous post about predicting your risk of a heart attack, the LDL-C value on your lipid panel is not measured directly, it’s estimated using the Friedewald equation:
LDL-C = Total Cholesterol - HDL Cholesterol - (Triglyceride / 5)Your LDL-C (LDL-calculated) estimates the mass of cholesterol carried by LDL particles in one deciliter of blood. There are several limitations to this estimate:
- Inaccurate at high and low triglyceride levels (> 400 mg/dL or <100 mg/dL)
- Assumes that the ratio of Triglycerides to vLDL cholesterol is 5:1, which isn’t always true
- Ignores cholesterol carried by other atherogenic particles: vLDL, IDL, and Lipoprotein(a)
ApoB vs LDL cholesterol
ApoB is more accurate measure of cardiovascular risk than LDL cholesterol. Evidence shows that the number of atherogenic particles is a better predictor of cardiovascular risk than the cholesterol mass LDL particles. Since even cholesterol-poor LDL particles can be harmful when there are many of them, LDL-C can be an incomplete measure.
Since each atherogenic lipoprotein has exactly one ApoB molecule, measuring ApoB provides a direct count of atherogenic particles, and is therefore considered a more accurate measure of cardiovascular risk. More particles = more chances to enter artery walls = higher risk of a blockage.
ApoB vs non-HDL cholesterol
Non-HDL cholesterol is calculated as Total Cholesterol - HDL. ApoB also measures heart disease more accurately than non-HDL cholsterol. A 2012 meta-analysis of 233,455 patients found ApoB predicted cardiovascular events about 13% better than non-HDL cholesterol. Why? Non-HDL cholesterol still measures cholesterol mass rather than particle number, which is the key driver of atherogenesis.
When ApoB and LDL disagree (discoradance)
ApoB, LDL, and non-HDL cholesterol are often aligned, but discordance has been found in many scenarios. For example:
- Men, Hispanics, older patients, statin users, and patients with high triglycerides or high BMI showed more discordance (2024 study)
- 20% of women had discordance in this 2017 study
The 2016 CARDIA study quantified the value of ApoB over LDL-C when they diverge. It assessed long-term cardiovascular risk by measuring LDL and ApoB levels in adults aged 18–30, then measured coronary artery calcification (CAC)—a marker of plaque buildup—via CT scan 25 years later. The study found young adults with high ApoB and normal LDL-C had 55% higher odds of developing CAC in the future. Those with high LDL-C and normal ApoB did not show a statistically significant increase in CAC risk.
Source: “Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification: The CARDIA Study”, Wilkins et al.
We see similar patterns in Empirical Health’s own data. Among 1,710 patients who had both LDL and ApoB measured, the two metrics agreed most of the time (r=0.91)—but in 10% of cases, they disagreed. 8% of patients had elevated ApoB (≥100 mg/dL) despite normal LDL (<130 mg/dL), meaning their cardiovascular risk would have been missed by a standard lipid panel. Only 2% had the reverse pattern of elevated LDL with normal ApoB.
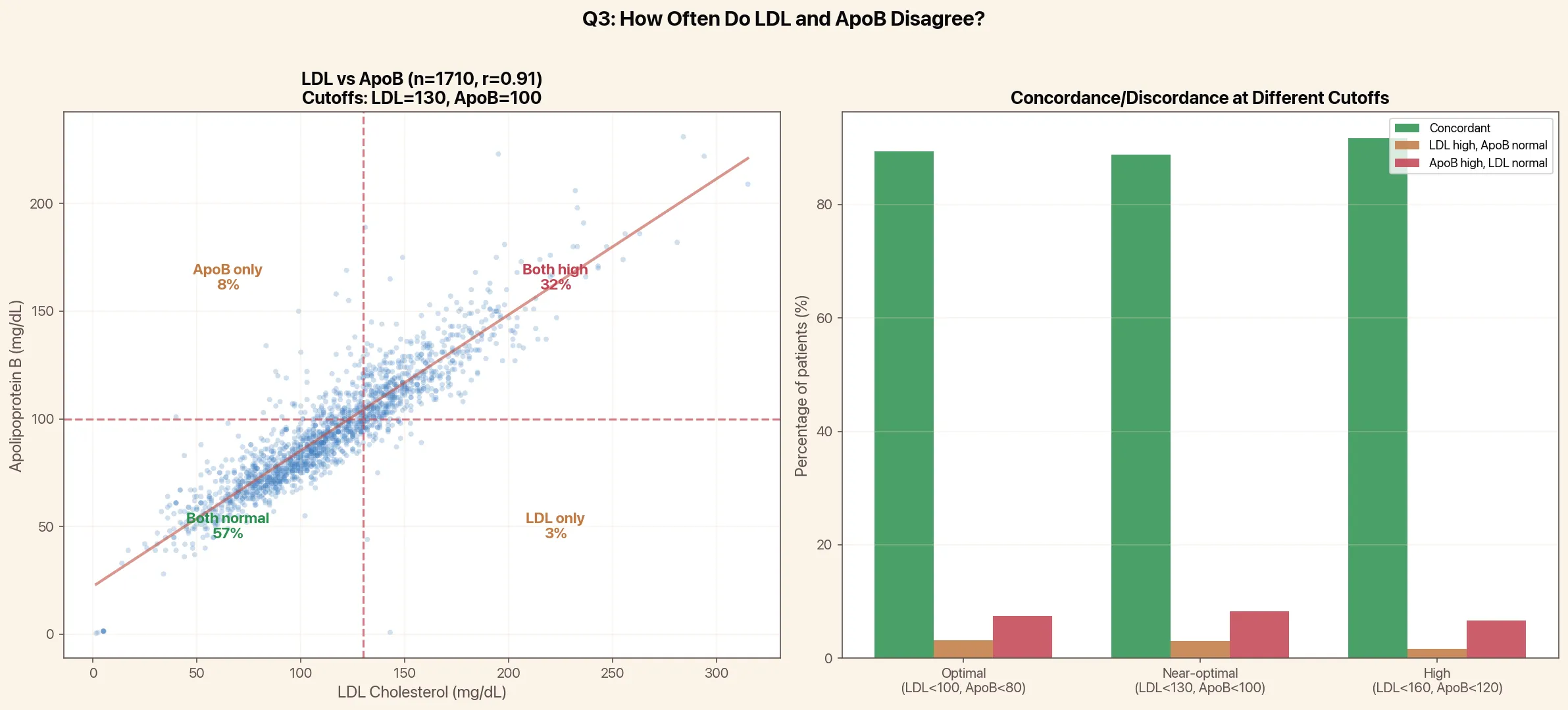
ApoB vs LDL-C concordance and discordance among 1,710 Empirical Health patients. Left: scatter plot showing correlation (r=0.91) with cutoffs at LDL=130 and ApoB=100 mg/dL. Right: discordance rates at different risk thresholds. Source: Empirical Health data.
Although LDL-C and ApoB are often aligned, when they are not, ApoB is the better predictor of heart disease risk.
Can you have high LDL and low ApoB?
Yes. In a (2021 study), 51% of patients with metabolic syndrome had high LDL-C but normal ApoB. High LDL with low ApoB can happen partly because triglycerides affect the measurement of LDL-C, but not ApoB.
Normal range of the ApoB test
ApoB target levels depend on your cardiovascular risk. The 2026 AHA/ACC dyslipidemia guidelines now include specific ApoB goals alongside LDL-C targets:
| Risk Level | Who this applies to | ApoB Target | LDL-C Target |
|---|---|---|---|
| Very-High Risk | Clinical ASCVD at very high risk, severe hypercholesterolemia with clinical ASCVD, CAC ≥1000 AU | < 55 mg/dL | < 55 mg/dL |
| High Risk | Clinical ASCVD not at very high risk, PREVENT-ASCVD ≥10%, diabetes with risk factors, CAC ≥100 AU | < 70 mg/dL | < 70 mg/dL |
| Moderate Risk | PREVENT-ASCVD 3–<10%, diabetes without additional risk factors, severe hypercholesterolemia without ASCVD | < 90 mg/dL | < 100 mg/dL |
The European Society of Cardiology (ESC) has similar targets: <65 mg/dL for very-high risk, <80 mg/dL for high risk, and <100 mg/dL for moderate risk.
In other words, a normal ApoB level is between <55 mg/dL and <90 mg/dL, depending on your other risk factors.
Does insurance cover ApoB testing?
Most health insurance doesn’t cover universal ApoB testing. Medicare’s ApoB testing policy “denies coverage for all CV risk assessment panels, except the basic lipid panel.” Some private insurers, like United Healthcare, cover ApoB in certain circumstances like high tryglerides, diabetes, obesity or metabolic syndrome, for people on lipid therapy, and so on Hypertriglyceridemia (detailed policy.
What ApoB level does Peter Attia recommend?
Note: Empirical Health is not affiliated with Peter Attia
While the ESC and National Lipid Association recommend an ApoB of <100 mg/dL, some advocate for an even lower level. Peter Attia advocates for an ApoB of <60 mg/dL (5th percentile of the population). If possible, he advocates getting it even lower, to about 20-30 mg/dL, although that may not be practical for everyone. Typically, lowering your ApoB to <60 mg/dL would require not only diet and exercise, but also stacking multiple medications (e.g., statins plus PCSK9 inhibitors). Reaching the 5th percentile may not be practical for everyone due to sheer cost (about $5,850 per year for PCSK9 inhibitors). Reaching the 20th percentile of ApoB, about 78 mg/dL, is achievable for most with inexpensive medications. Reaching below the median ApoB, 97 mg/dL, is still beneficial and corresponds to the ESC and National Lipid Association guidelines above. Peter Attia generally doesn’t recommend an ideal LDL cholesterol: instead he recommends measuring ApoB.
How to lower your ApoB naturally
The good news is that you can reduce your ApoB through nutrition:
- Increase soluble fiber
- Reduce saturated fat
- See also: how to lower your cholesterol in 7 days and normal cholesterol levels for ApoB and LDL targets
(Surprisingly, dietary cholesterol does not have a strong effect on the number of atherogenic particles for most people.)
The mechanism for how your diet affects your ApoB is related to cholesterol metabolism. Your liver extracts ApoB-containing lipoproteins from your blood and uses them to create bile acid. During digestion, these bile acids are secreted into your gut to help break down fats. 95% of bile acids are then reabsorbed so they can be reused.
Eating soluble fiber disrupts this cycle. In the gut, soluble fiber absorbs water and thickens into a gel. This gel physically traps bile acid, prevents it from being reabsorbed back to your liver, and it gets excreted. Your liver then senses less bile acid, so it breaks down more ApoB-containing lipoproteins from your blood to replenish.
Eating saturated fat has the opposite effect. Saturated fats are broken down and absorbed in the gut before reaching the liver. This causes the liver to increase production of vLDL (and eventually LDL) and also reduce the clearing of atherogenic lipoproteins from the blood.
How to lower your ApoB with medication
The primary medications to reduce ApoB are statins. Statins decrease your liver’s synthesis of cholesterol and increase your liver’s removal of LDL particles from the blood. The most common is Atorvastatin (Lipitor), with over 100 million prescriptions filled in the U.S. each year. Statins are remarkably effective, with severe patients seeing a 20-40% reduction in ApoB in just a few months, inexpensive (~$5/mo), and safe, with the most common side effect (muscle pain) occurring in <1% of patients.
How can you measure your ApoB levels?
Empirical Health’s advanced cardiovascular panel includes ApoB testing, along with a complete lipid panel, and Lipoprotein(a), which is an atherogenic lipoprotein primarily determined by genetics.

What’s the cost of an ApoB lab test?
You can get an ApoB test for $190 as part of an advanced cardiovascular panel. The panel includes 100 biomarkers, requires a single blood draw at one of 2,000 testing sites. Most results come back within a couple days. You can get the advanced cardiovascular panel within the Empirical Health app for iPhone and Android, or you can order the advanced heart health panel here.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
