The American Heart Association and American College of Cardiology just released the first update to cholesterol guidelines in eight years. The new 2026 guidelines make 52 distinct new recommendations on heart health, cholesterol, cardiac imaging, medications, and so on.
The biggest changes are:
- Lp(a) testing is now recommended for all adults. Lp(a) is the strongest hereditary risk factor for heart disease.
- Treatment is now recommended for younger adults, based on 30-year heart disease risk projections rather than 10-year risk.
- ApoB testing, hsCRP (inflammation), and CAC (imaging) are recommended more frequently. These are essentially better biomarkers for heart health.
- Specific LDL targets are back, after being removed in the 2013 guidelines.
In this post, we’ll describe each of these changes, and some of the evidence behind them.
How the AHA/ACC classifies evidence
The ACA/ACC classifies evidence into two axes: the magnitude of the effect, ranging from class 1 (strong yes) to 3 (neutral or harmful), and the strength of the evidence, ranging from A (multiple randomized control trials) to C (weaker evidence like observational data, expert opinion, or mechanistic studies). Level B is intermediate quality evidence, which is divided into B-R (randomized) vs B-NR (nonrandomized).
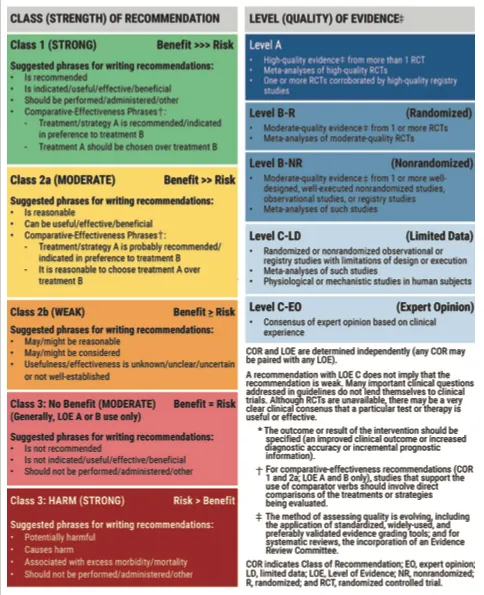 How to read AHA/ACC recommendations: Class of Recommendation (strength) and Level of Evidence (quality) are two separate axes. A “Class 1, Level B” recommendation means the benefit strongly outweighs risk, based on moderate-quality evidence. Source: 2026 ACC/AHA Dyslipidemia Guideline.
How to read AHA/ACC recommendations: Class of Recommendation (strength) and Level of Evidence (quality) are two separate axes. A “Class 1, Level B” recommendation means the benefit strongly outweighs risk, based on moderate-quality evidence. Source: 2026 ACC/AHA Dyslipidemia Guideline.
Lp(a) testing is now recommended for all adults
Lp(a), or Lipoprotein (a), is a type of cholesterol particle that is “stickier” than normal cholesterol. One study estimates each Lp(a) particle is 6.6x more atherogenic than normal cholesterol.
The AHA and ACC now recommend every adult test their Lp(a) at least once. This is a Class 1 recommendation, the strongest. It’s a major change from the 2018 guidelines, which mentioned Lp(a) only as a “risk enhancer” without a specific testing recommendation.
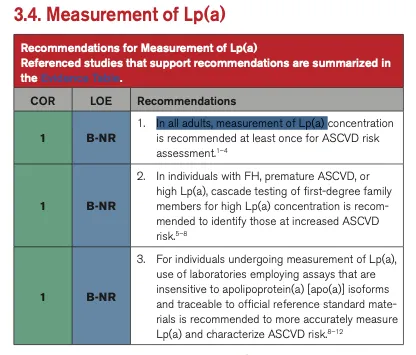 The 2026 guidelines now recommend universal testing of Lipoprotein (a). Source: 2026 ACC/AHA Dyslipidemia Guideline.
The 2026 guidelines now recommend universal testing of Lipoprotein (a). Source: 2026 ACC/AHA Dyslipidemia Guideline.
Lp(a) is the strongest inherited risk factor for heart disease. About 20% of people have elevated levels (≥125 nmol/L or ≥50 mg/dL), which increases ASCVD risk by about 40%. At very high levels (≥250 nmol/L), risk doubles. And because Lp(a) is almost entirely genetic and remains stable throughout your life, one measurement is enough.
The guidelines also recommend cascade testing. If you have high Lp(a), your first-degree family members (parents, siblings, children) should be tested too.
| Lp(a) level | Relative ASCVD risk increase |
|---|---|
| <75 nmol/L (<30 mg/dL) | Reference (low) |
| 75–124 nmol/L (30–49 mg/dL) | 1.2× |
| ≥125 nmol/L (≥50 mg/dL) | 1.4× |
| ≥250 nmol/L (≥100 mg/dL) | 2× |
| ≥350 nmol/L (≥150 mg/dL) | 3× |
| ≥430 nmol/L (≥180 mg/dL) | 4× |
Data from the UK Biobank Study, as cited in the guideline.
The guidelines also endorse ApoB for many patients. In about 20% of people, LDL-C can look normal while ApoB is elevated (meaning their actual risk is higher than it appears). The guideline notes that “only apoB remains significant” as a predictor of heart attacks when assessed alongside other lipid markers. (In other words, you do not need to test cholesterol particle sizes.)
Treating cholesterol earlier in the young
Previous guidelines focused on 10-year risk of a heart attack, but we know that damage to your arteries accumulates over your lifetime. As Dr. Steven Nissen of Cleveland Clinic puts it, “time-averaged LDL cholesterol over your lifetime is one of the strongest predictors of whether you’re going to have a heart attack, stroke or sudden death.”
The 2026 guidelines change both the equations used to predict risk (including a 30-year option), and the treatment guidelines (lowering cholesteorl exposure for less time).
A new risk calculator: PREVENT replaces the Pooled Cohort Equations
The 2018 guidelines used the Pooled Cohort Equations (PCE) to estimate 10-year heart disease risk. The 2026 guidelines replace PCE with the PREVENT-ASCVD equations, which give 10-year and 30-year risk estimates.
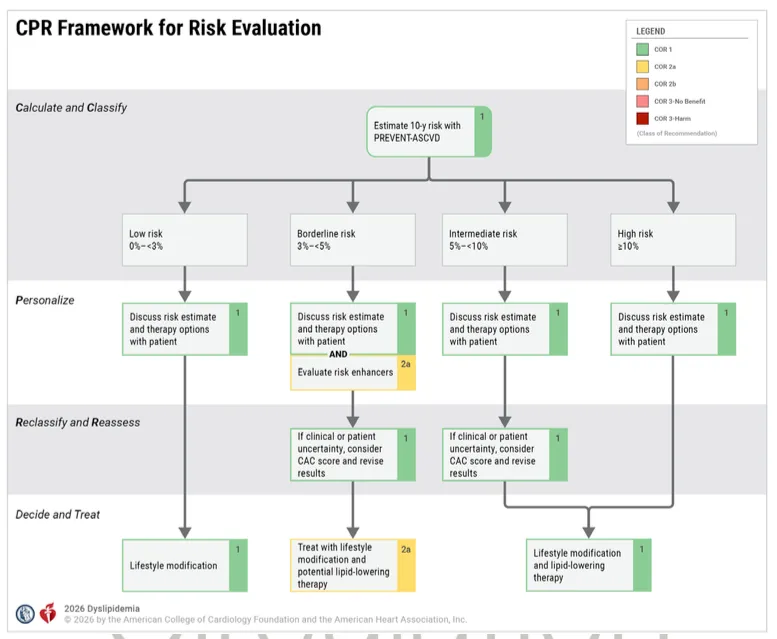 The “CPR” framework: Calculate risk with PREVENT, Personalize by discussing with your doctor, and Reclassify with CAC scoring if needed. Source: 2026 ACC/AHA Dyslipidemia Guideline.
The “CPR” framework: Calculate risk with PREVENT, Personalize by discussing with your doctor, and Reclassify with CAC scoring if needed. Source: 2026 ACC/AHA Dyslipidemia Guideline.
PREVENT covers a wider age range (30–79 years vs. 40–75 for the old equations), incorporates kidney function, is race-free, and includes some social factors (like zip code). The 30-year risk estimates especially affect younger adults, where 10-year risk may look low but lifetime exposure is high. The guidelines now recommend statin therapy for young adults (≤30 years) with LDL-C ≥160 mg/dL or a strong family history of premature heart disease. Children ages 9–11 should be screened for cholesterol. For adults at low 10-year risk but with a 30-year risk ≥10%, a moderate-intensity statin is now considered reasonable.
Specific LDL-C targets are back
The 2026 guideliens include specific LDL-C treatment goals, something the ACC/AHA had moved away from in their 2013 guidelines. Here’s how LDL cholesterol target ranges break down by risk level:
Primary prevention (no existing heart disease)
| 10-year ASCVD risk | LDL-C goal | Non-HDL-C goal | Statin intensity |
|---|---|---|---|
| Low (<3%) | Lifestyle optimization | — | Generally not recommended |
| Borderline (3% to <5%) | <100 mg/dL | <130 mg/dL | Moderate-intensity reasonable |
| Intermediate (5% to <10%) | <100 mg/dL | <130 mg/dL | At least moderate; high for upper range |
| High (≥10%) | <70 mg/dL | <100 mg/dL | High-intensity recommended |
Secondary prevention (existing heart disease)
| Risk category | LDL-C goal | Non-HDL-C goal |
|---|---|---|
| ASCVD, not very high risk | <70 mg/dL | <100 mg/dL |
| ASCVD, very high risk | <55 mg/dL | <85 mg/dL |
The <55 mg/dL target for very-high-risk patients aligns with what the European Society of Cardiology recommended in 2019, and is now endorsed by the ACC/AHA for the first time.
New heart disease treatments available since 2018
Since the last guideline, several new lipid-lowering medications have received FDA approval and are now incorporated into the treatment recommendations:
Bempedoic acid (Nexletol)
An oral medication that lowers LDL-C by 21–24% as monotherapy (17–18% when added to a statin). It works upstream of statins in the cholesterol synthesis pathway. The CLEAR OUTCOMES trial showed it reduces cardiovascular events in patients who can’t tolerate statins—making it an important option for the roughly 10% of patients with statin-attributed muscle symptoms. It’s a prodrug activated in the liver, so it doesn’t cause the muscle side effects associated with statins.
Inclisiran (Leqvio)
A small-interfering RNA (siRNA) therapy that silences the gene for PCSK9, the protein that degrades LDL receptors. Some people naturally have a PCSK9 mutation, and have low LDL cholesterol, ~80–90% lower lifetime risk of coronary heart disease, and no apparent negative side effects. Inclisiran was essentialy designed to give that mutation to the rest of us. It’s injected just twice a year (after two initial doses) and lowers LDL-C by 48–52%. This is a major convenience improvement over the existing PCSK9 monoclonal antibodies (evolocumab and alirocumab), which require injections every 2–4 weeks. Cardiovascular outcomes trials are still in progress, so the guidelines recommend inclisiran primarily when patients can’t tolerate or obtain the existing PCSK9 antibodies.
Evinacumab and Olezarsen
These are approved for rare conditions familial hypercholesterolemia (HoFH) and familial chylomicronemia syndrome (FCS). Most people won’t need them, but they’re very handy for people who do.
The guidelines lay out a clear escalation pathway for patients who don’t reach their LDL-C goals (see also: how to lower your ApoB): 1. Start with a statin, 2. Add ezetimibe if LDL-C goal is not met, 3. Add a PCSK9 monoclonal antibody** (evolocumab or alirocumab) or bempedoic acid, 4. Consider inclisiran if PCSK9 antibodies aren’t tolerated or accessible.
For patients with elevated Lp(a) and established ASCVD, the guidelines specifically recommend adding a PCSK9 monoclonal antibody, which is the only available therapy with proven cardiovascular benefit that also lowers Lp(a). (Four Lp(a) specific medications are in clinical trials today, and are likely to be approved in the next coupel of years.)
What the new heart health guidelines mean for cholesterol testing and treatment
The key takeaway from the 2026 guidelines is that the standard lipid panel is no longer sufficient for understanding your cardiovascular risk. The AHA/ACC now recommends that every adult get Lp(a) tested at least once, and that ApoB and hsCRP be used to guide treatment decisions—especially in patients with diabetes, elevated triglycerides, or existing heart disease. If you haven’t had your Lp(a) measured, these guidelines say you should. And if your LDL-C looks fine but you have diabetes, metabolic syndrome, or a family history of heart disease, an ApoB measurement could reveal hidden risk.
Empirical’s comprehensive heart panel includes ApoB, Lp(a), and the other biomarkers now emphasized by the AHA/ACC, available direct-to-consumer for $190.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
